

Diagnostic errors in imaging are prevalent; most retrospective reviews have determined that the average error rate for radiologists is 3 to 37%, depending on the modality and disease process studied. Fortunately, most of these errors do not negatively impact patient care. However, given the high volume of imaging in the US alone each year, it turns out the radiologists are one of the most frequently sued physicians for failure to diagnose or delay to diagnose – typically the consequence of a missed finding. According to a Coverys report analyzing 10,618 closed medical professional liability claims over a 5 year period, radiologists were the third most frequent group in terms of a number of diagnosis-related claims with 14% after general medicine (24%) and the hospital/facility (19%). The good news is that once you understand why errors occur, you can then take steps to prevent them from happening. That will be the focus of this blog.
Before presenting my 4 tips to reduce errors and improve efficiency in radiological interpretation, I would like to share my background. I have been practicing radiology in various roles for about the last 10 years after completing residency and fellowship training at Penn Medicine in Abdominal Imaging. I held academic positions for 8 years as a “body radiologist”, then transitioned into general practice teleradiology working for various groups over the last 2 years with a continued focus on cancer imaging. During this time, I have held a number of administrative and leadership roles at the local and national levels, including Vice-Chair of Operations and Vice-Chair of Quality. I was part of the committees that crafted the ACGME Milestones for resident and abdominal imaging fellows. I have published over 50 papers in the peer-reviewed literature, many of which are about errors and interventions to reduce them. Over the last 5 years, I have consulted on between 40-50 medical malpractice cases for both plaintiffs and defendants involving imaging, providing opinions about Standard of Care and Causation. It is this experience I am drawing upon to provide the key tips.
Tip #1: Follow up on your cases, as many as you can. Whether it’s a notecard in your scrub pocket or a password-protected access database, jot down every time you see an interesting case, particularly if you expect there to be surgery, pathology, or follow-up imaging. There is a whole field of research that focuses on how experts develop “expert intuition”, or the ability to quickly and accurately arrive at the correct diagnoses in complex scenarios when less experienced professionals cannot (Naturalistic Decision-Making, check out Sources of Power by Gary Klein). One of the two criteria for developing expert intuition is the feedback that is frequent, timely, and accurate. This will hone your diagnostic skills, improving accuracy and reducing errors. It will also make you faster and more efficient in interpretation.
Tip #2: Get involved in peer review at your training program or practice. The goal is to see as many error cases as possible. The more errors you see, the less likely you are to make the same error. I can tell you what happens when you’ve seen a particular type of error several times – you no longer have to actively look for it, your eyes are drawn to it. I’ve gotten to the point both in clinical practice and when reviewing malpractice cases that if it’s a miss I’m familiar with, my eyes simply jump to the finding when it is in my field of view. Every miss is a pearl that we all can learn from.
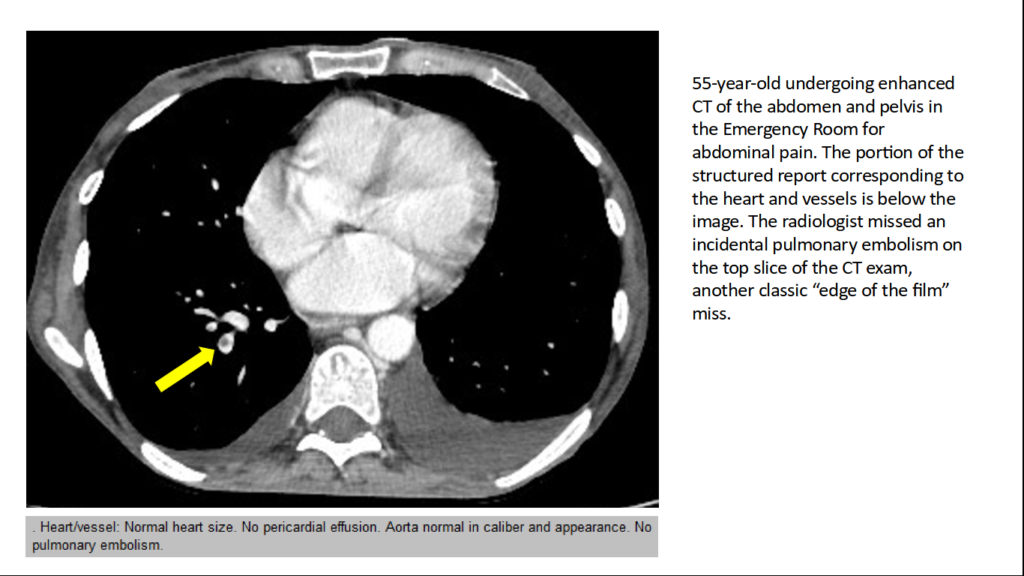
Tip #3: Optimize your search pattern for blind spots. Whether you specialize in body imaging, neuroradiology, or are a jack of all trades (general radiologist), there are several publications in the radiology literature highlighting blind spots. I can list common blind spots in the abdomen and pelvis; abdominal wall (metastases, desmoids, endometrial implant in c-section scar), pedicles of the spine (bone metastases), paravertebral soft tissue (tumors/metastases and early paraspinal abscess), lower lobe pulmonary arteries (incidental pulmonary embolism), peritoneal surface (peritoneal implants), and perianal region (perianal abscess and fistula). If you have a blind spot, consider updating your templates and using them as a checklist. And keep the template fields empty – templates are less effective as a checklist when the fields are pre-filled.
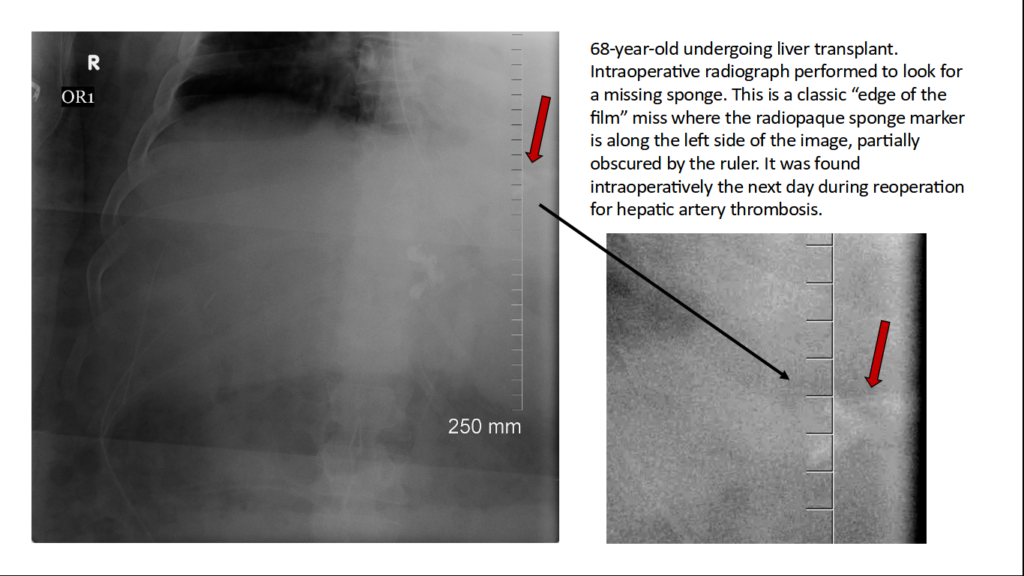
Tip #4: Learn about cognitive biases. Have you heard the terms framing bias, alliterative error, edge of the film miss, and satisfaction of search? Cognitive biases arise from the way our minds make decisions in the interpretation of imaging studies and can result in systematic errors in interpretation.
There are more than 40 types of cognitive biases, which contribute to approximately 30% of radiological misses. When you are familiar with why cognitive biases occur, you are less likely to make these types of errors and subsequently be an unwilling contributor to one of my articles about misses.
If you found the content of this blog helpful, you can visit my website to see 12 lectures about diagnostic errors. My next blog will be about lessons learned from medical malpractice cases.